





Small number of RAC homes that used paper records failed accreditation standard on information systems. Six risk indicators for an RAC home to fail the information systems outcome were identified. Reports from the Aged Care Standards and Accreditation Agency produced between April 2011 and December 2013. Items identified included types of information systems, compliance with accreditation standards, and indicators of failure to meet an expected outcome for information systems. The Impact of Electronic Health Records on Risk Management of Information Systems in Australian Residential Aged Care Homes.
Keywords: Risk Management Impact EHR Aged Care
Despite the potential of electronic health records (EHR) to significantly improve the quality of information management in comparison with paper-based records, there are limited reports of the actual benefits of EHR for information management in residential aged care. In a qualitative research study with focus-group data collection, Cherry et al. found that the managers in long-term care homes with EHR usage experience perceived these systems to be more efficient than paper records, giving improved quality and accuracy of documentation. They provide easier access to charts and resident care information. They also improve management ability to monitor resident care activities and initiate improvement actions, and better resident outcomes related to improved documentation quality.
Based on a publication of the US Institute of Medicine, we define aged care EHR in this study as a repository of aged care service recipients’ data in digital form. Aged care EHR contains retrospective, concurrent, and prospective longitudinal electronic health and aged care service information pertaining to a care recipient. They are accessible by multiple authorised users. EHR are generated and maintained by aged care service providers with the primary purpose of giving continuing, efficient and safe health and aged care for their clients. The functionality of EHR may include demographic information, admission assessment, care planning, on-going assessment, nursing charts, progress and incident reporting care planning, medication management, ongoing assessment, nursing charts, progress and incident reporting.
Electronic Health Records improve the quality and efficiency of information management
Increasing number of RAC homes in Australia and the United States have been introducing EHR systems over the last decade. The reasons are to standardise the structure and process of client record keeping, and improve the quality and efficiency of information management. These changes are expected to increase the quality-adjusted life years of the older people and improve health decision-making, and access to patients’ medical history., EHR systems should also provide better evidence that care services meet nursing and accreditation standards and legal requirements.
After using EHR systems for up to two years, care staff in nine Australian RAC homes perceived the benefits of EHR to them include quick data entry and retrieval, improved format and content of records, facilitating internal and external communication, and better understanding of residents’ requirements. Unintended adverse consequences included difficulties for some staff in data entry and information retrieval, resistance to using the system, increased complexity of information management, and end-user concerns about access. Reasons included the nature of the EHR systems and the ways the systems were implemented and used by nursing staff.
A nursing documentation audit in seven Australian RAC homes provided information on key differences between the electronic and paper record formats. Nursing care plans in the EHR system documented more signs and symptoms of resident problems and evaluation of care than the paper-based plans, but had a lower mean quality score. The EHR plans contained fewer problem or diagnosis statements, contributing factors and resident outcomes than the paper-based system. Both types of nursing care plan were weak in documenting measurable and concrete resident outcomes. The overall quality of documentation content for the nursing process was no better in the electronic system than in the paper-based system.
 Risk Management Impact of EHR in Aged Care
Risk Management Impact of EHR in Aged Care
Article in Journal of Medical Systems · September 2016 DOI: 10.1007/s10916-016-0553-y: Ping Yu
However, despite the potential of EHR to significantly improve the quality of information management in comparison with paper-based records, there are limited reports of the actual benefits of EHR in RAC. Therefore, the aim of this study was to identify any differences in meeting aged care accreditation requirements between the RAC homes that used EHR for information management and those that used paper records. The hypothesis to be tested is that the RAC homes using EHR have better performance in meeting information system standards in aged care accreditation than those that use paper records for information management. This analysis will help us understand the contribution of EHR in managing risks for information management in Australian residential aged care (RAC) homes.
Aged Care Accreditation in Australia
The Australian government implements a comprehensive accreditation system through the Australian Aged Care Quality Agency (AACQA), which determines whether the aged care services provided by an RAC home meet the relevant safety standards. AACQA commenced operation in 2014, superseding the Aged Care Standards and Accreditation Agency (ACSAA).
The accreditation process in Australia involves self-assessment by RAC homes against the accreditation standards and the submission of an application for accreditation. This is followed by a desk audit and a site audit by a team of registered aged care quality assessors. A person is only qualified as a registered aged care quality assessor after completing approved training and orientation of aged care accreditation. When auditing an RAC home, the assessors are required to observe the Code of Conduct and to have no pecuniary or other interest that may conflict with a proper audit. Given the high standards of performance and integrity required in aged care accreditation, the report produced by the assessors after a site visit is treated as valid and reliable official report of the AACQA. A decision about the home’s accreditation, either meeting or not meeting the standards, is then made by AACQA based on the self-assessment by the RAC home, desk audit and site audit. Finally, an accreditation certificate is issued, as well as the accreditation report.
According to the Australian Aged Care Act, RAC homes are required to meet the accreditation standards at all times and ensure the safe care of residents. When a home fails to meet the standards, AACQA may put the home on a time-table for improvement (TFI), which sets out the required improvements and the maximum time allowed for addressing those expected outcomes that were not met. By the end of the timetable, the AACQA will arrange for assessors to conduct a review audit. If the standards are still not met, the home’s accreditation will be varied or revoked. The Department of Health may also decide to impose sanctions on the home. Therefore, meeting aged care accreditation standards is the basic safety requirement imposed by the Australian government on a RAC home in aged care service provision.
There are four RAC accreditation standards in Australia:
-
- Management systems, staffing and organisational development;
- Health and personal care;
- Care recipient lifestyle; and
- Physical environment and safe systems.
Article Keywords: Risk Management Impact EHR Aged Care
Each standard includes a series of expected outcomes. There are 44 of these outcomes across the four standards with which an RAC home must comply at all times in order to meet accreditation requirements. Common to all four standards are the outcomes of continuous improvement, regulatory compliance, education and staff development. The Principle of Standard One is to be responsive to the needs of residents, their representatives, staff and stakeholders, and the changing environment in which the service operates. The six outcomes that are specific to Standard One are comments and complaints, planning and leadership, human resource management, inventory and equipment, information systems and external services.
The requirement for outcome 1.8, information systems, which was a focus for this study, is that ‘Effective information management systems are in place’.
The publicly available RAC accreditation reports provide the most objective and authoritative information on whether an RAC home meet the accreditation outcome of 1.8 information systems The reports also contain information about the type of records used in an RAC home, being EHR or a paper records-based system. By analysing the information in Section 1.8 of the accreditation reports, it is possible to infer which indicators of ‘effective information management systems’ were used by the accreditation agency and whether these had differed between RAC homes that used EHR and those that had paper-based records. Therefore, our approach to address the research question was to conduct a comprehensive analysis of Australian aged care accreditation reports.
Effective information management systems Methods
We followed a four-step process to extract and analyse data from these reports:
- data sourcing and processing,
- data cleaning, data restructuring and
- labelling, and analysis.
Data Sourcing and Processing
Data were sourced from the website of the Aged Care Standards and Accreditation Agency in December 2013. We downloaded 2,754 aged care accreditation reports that were produced from 27 April 2011 to 3 December 2013.
We converted the original reports in PDF format to computer-program readable text formats (e.g. .txt files) using software Adobe Acrobat Pro. We extracted the relevant sections in all reports, including 44 expected accreditation out-comes and Outcome Information Systems into text files.
Data Cleaning
The first author manually compared the converted text files with the original PDF documents for 2,754 reports. The incorrect character encoding was concentrated on list characters like ‘’ in PDF format. These were converted to ‘?’ or ‘????’ in txt format. Otherwise, the errors did not influence reading the content.
Data Restructuring and Labelling
Data were labeled according to two criteria: failing to meet one or more aged care accreditation outcomes, and using some form of EHR. First we identified the RAC homes that failed to meet one or more aged care accreditation outcomes by searching the content such as that presented in Table 1busing the keyword ‘not met’.
To identify the RAC homes that used an EHR system and those used paper records, first we read through 50 copies of the accreditation reports and found that different terms were used to describe an electronic record system. Based on the terms we identified, we developed a list of keywords that was used to identify whether an RAC home used an EHR system or paper records. They included electronic clinical plan, electronic clinical documentation, electronic clinical in-formation, electronic documentation, electronic care plan, electronic care documentation, electronic care information and electronic health record.
We scanned section 1.8 Information Systems in the reports (see Fig. 2b), and a list of documents that a RAC home submitted to the accreditation agency for desk audit. Based on this, we used a program to automatically structure the name of an RAC home (from document name), frequency of matching the keywords and details of matching (e.g. 30 characters before and after each keyword) into an Excel spreadsheet (Table 1). The reliability of the labels in Table 1 was further validated by manual checking against the original documents.
Afterwards, we aggregated all RAC homes into four groups:
- Group 1 – meeting all accreditation standards and using EHR,
- Group 2 – meeting all accreditation standards and using paper records,
- Group 3 – not meeting one or more accreditation standards and using EHR, and
- Group 4 – not meeting one or more accreditation standards and using paper records.
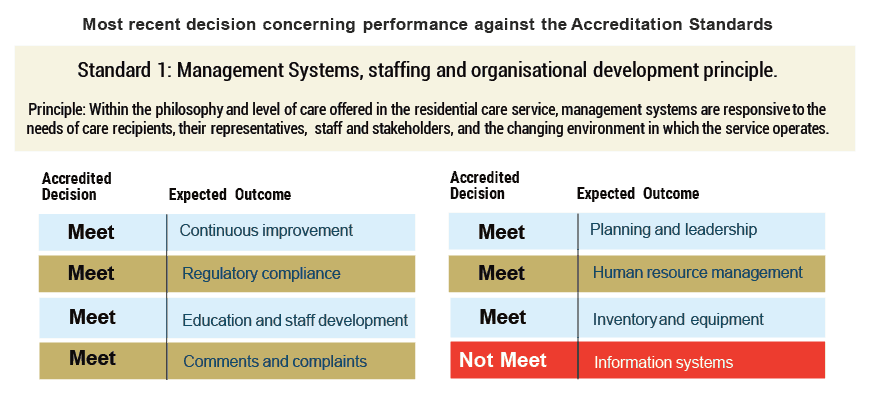 Fig. 1 a – Risk Management Impact EHR Aged Care
Fig. 1 a – Risk Management Impact EHR Aged Care
Fig. 1 a- An example of the expected accreditation outcomes for Standard 1 in the accreditation report.
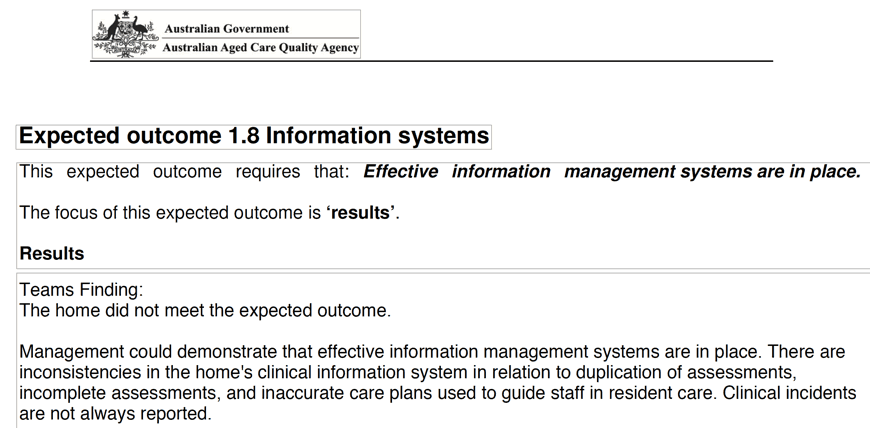 Fig. 2 a – Risk Management Impact EHR Aged Care
Fig. 2 a – Risk Management Impact EHR Aged Care
Fig.2 a–An example of findings for Outcome 1.8 Information Systems in the original accreditation report in PDF format.
Risk Management Impact EHR Aged Care: Data Analysis
Both quantitative and qualitative data analyses were conducted in this study. Pearson’s Chi-square test was used to identify differences between the four groups of the RAC homes –those that used EHR systems or used paper records in meeting or not meeting aged care accreditation standards. The level of significance was set at p = 0.05.
Qualitative content analysis was conducted to identify and classify the indicators for not meeting accreditation Outcome 1.8 Information Systems. This enabled us to identify the statements that described the reasons for failing to meet this out-come. We compared these statements with the contributions of EHR to residential aged care suggested by the previous studies.
Risk Management Impact EHR Aged Care: Results
Thirteen RAC homes were found to not meet one or more accreditation standards. These RAC homes and the relevant accreditation outcomes that at least one RAC home did not meet are listed in Table 2.
Difference in Meeting Accreditation Standards between RAC Homes Using EHR and Those Using Paper Records
Of the 2,754 RAC homes audited, 1,031 (37.4%) used an EHR system for client health and personal care information management and 1,723 (62.6%) used only paper records. Only 13 homes (0.5%) failed to meet one or more of the 44 accreditation outcomes. One of these homes used an EHR system and met requirements for Outcome 1.8. Of the twelve homes that used paper records, nine failed in Outcome 1.8 (see Fig. 3).
The result of the Chi square test suggested that the proportion of RAC homes using EHR that met accreditation standards (99.9%) was significantly higher than that of their counterparts using paper records (99.3%, p = 0.026).
Risk Indicators for Failure to Meet Outcome 1.8 Information Systems
Six risk indicators were identified in the reports for the nine RAC homes using paper records that failed to meet the information system outcome (Table 3). Staff in six homes did not have access to accurate and appropriate information (R1). Monitoring mechanisms were not effective in identifying deficiencies in information systems in four homes (R2). Two homes did not always report clinical incidents (R3). There were insufficient records of residents’ clinical changes in two homes (R4). One home failed to produce accurate care plans (R5) and one home’s communication processes were not effective (R6). These deficiencies led the agency to conclude that these RAC homes did not have effective information systems.
Risk Management Impact EHR Aged Care: Discussion
This study aimed at identifying the contribution of EHR to managing risks for information system accreditation in RAC homes. We found that EHR systems had already been adopted by 37.4% of 2754 RAC homes. Thirteen RAC homes did not meet all expected outcomes in the Australian standards. Of these, nine out of 12 that used paper-based records failed the outcome for information systems. Through analysis of the records for these nine homes, we identified six risk indicators in information systems, which were used by the accreditation agency to decide that the information system accreditation outcome had not been met. This provided insight about the areas of information system management to which RAC homes may need to pay attention and continuously improve.
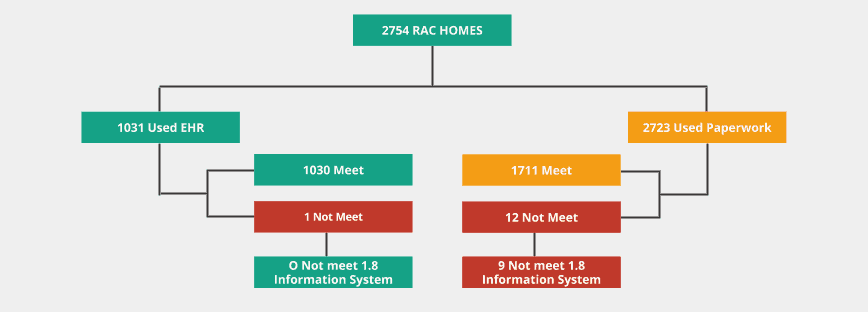 Fig. 3 – Risk Management Impact EHR Aged Care
Fig. 3 – Risk Management Impact EHR Aged Care
Fig. 3 An outline of the RAC homes that used EHR or paper records, met or did not meet the accreditation outcomes, and whether they met or did not meet the accreditation Outcome 1.8 Information Systems
The study findings indicate that the overall contribution of EHR to meeting aged care accreditation standards in Australia was very small. Only 9 (0.3%) RAC homes failed the information system outcome. This may cause stagnation in the adoption of EHR by the rest 62.6% of RAC homes that were still using paper records by the end of 2013. The further adoption of EHR in Australian RAC sector needs to be continuously followed. However, none of the RAC homes that used EHR for information management failed to meet that outcome. Also, the proportion of RAC homes using EHR that met all accreditation standards was significantly higher than that of homes with paper records.
The aged care accreditation system in Australia is established to ensure an RAC service meets the minimum safety standard mandated by the Aged Care Act. It is not a quality ranking system, such as a star ranking system for e-Bay, which is available to the general public, thus providing the pressure and incentive for the aged care service providers to improve services. This explains why only 0.3% of RAC homes in this study failed the standard. Therefore, there is a lack of policy incentive for RAC homes in Australia to further improve quality once the minimum safety standard audited by the aged care accreditation system is met. This may cause inertia in the whole sector and stagnation in innovation, which needs to be further confirmed and studied.
Nevertheless the strength of this study is that it had the advantage of a nationwide overview of the performance of Australian RAC homes in information management and the possible contribution of EHR to this process. We believe it provides some indication of the benefits from EHR in RAC, consistent with those found in previous studies using other methods.
An inevitable limitation is that what we have reported is an association between EHR and accreditation, rather than decisive evidence that use of EHR is a reason for RAC homes to perform better in accreditation. Also, the sample size for de-tailed analysis of risk factors for failing to meet accreditation standards is small. Another limitation of the study is it does not provide information on practice details of the sort obtained from observational studies with small numbers of homes.
Risk Management Impact EHR Aged Care: Conclusion
This study identified six risk indicators for an RAC home to fail the information system accreditation standard in Australia. While a small number of RAC homes that used paper records failed accreditation standard on information systems, those that used EHR fully complied.
Risk Management Impact EHR Aged Care: References:
Article in Journal of Medical Systems · September 2016 DOI: 10.1007/s10916-016-0553-y
Ping Yu
Springer Science+Business Media New York 2016
Datanova e-business and e-commerce solutions
If you’re ready to optimise your business strategies, we offer cloud based CRM, eCRM, Social CRM, Case Management and self service customer portals:



FlowLogic: is not just software, it is a range of solutions designed to address the needs of Australian Community Care organisations.
FlowPoint: a cloud based portal preloaded with functions to engage and self-service your customers. Optimised for FlowLogic.
Want to see a demonstration of our solutions?
Let us show you how, Book a webinar.
Please call a Datanova Digital Business Solution Architect on 1300 552 166 and book your FREE Webinar alternatively send an email to Datanova. We will get back to you shortly.
Please call a Datanova Digital Business Solution Architect on 1300 552 166 and book your complimentary Webinar or alternatively send an email to Datanova. You can book a webinar straight from our booking form here and we will get back to you shortly.